

Abstract
Background: Positron emission tomography combined with computed tomography (PET-CT) has been widely used for initial staging and monitoring of treatment response in patients with malignant lymphomas. The predictive value of interim PET-CT (iPET) and end-of-treatment PET-CT (ePET) is well-established for patients with Hodgkin lymphoma, diffuse large B-cell lymphoma, and follicular lymphoma. However, there are limited data on their prognostic values in patients with mature T-cell and NK-cell lymphomas. In this study, we aimed to assess the value of iPET and ePET in the prediction of progression-free survival (PFS) and overall survival (OS) in patients with mature T-cell and NK-cell lymphomas.
Methods: Data of 99 patients with mature T/NK-cell lymphomas who underwent iPET (after 2-4 cycles of chemotherapy; performed just before the next cycle) or ePET at the Kameda Medical Center were retrospectively analyzed. PET-CT scans were scored as positive or negative based on the Deauville score using a 5-point scale. While a Deauville score of 1-3 was considered to indicate complete metabolic response (CMR) (negative), a score of 4-5 was considered as persistent or progressive disease (positive). Standardized uptake value (SUV) was normalized relative to the injected dose and lean body mass and was measured for all lesions. The highest SUV for each scan was recorded as maximum SUV (SUVmax). To quantitatively interpret iPET scans, we determined the rate of reduction in SUVmax between baseline and iPET (ΔSUVmax). Survival was calculated using the Kaplan-Meier method and compared using the log-rank test.
Results: In total, 99 patients, including patients with peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS) (n = 36), angioimmunoblastic T-cell lymphoma (AITL) (n = 28), anaplastic large cell lymphoma (ALCL) (n = 6), adult T-cell leukemia/lymphoma (ATLL) (n = 14), enteropathy-associated T-cell lymphoma (EATL) (n = 2), cutaneous T-cell lymphoma (CTCL) (n = 3), and NK/T-cell lymphoma (NKTCL) (n = 10), participated in this study. Of all patients, 55 (56%) were men, and the median age was 48 (range: 22-78) years. The majority of patients, except those with ATLL and NKTCL, were treated with CHOP or CHOP-like chemotherapy. After a median follow-up of 26 months, the 5-year PFS and OS rates for all patients were 24% and 41%, respectively. While 98 patients (99%) underwent iPET, 60 of them (61%) underwent ePET. Baseline PET-CT scan was positive in all cases, and the median SUVmax was 12.8 (range: 2.6-37.4). Using the ROC curve, ΔSUVmax values between baseline and iPET of >79% and >73% were predictive of better PFS and OS, respectively (PFS: sensitivity 77%, specificity 69%, area under the curve [AUC] 0.82, 95% confidence interval [CI] = 0.68-0.88 and OS: sensitivity 78%, specificity 63%, AUC 0.78, 95% CI = 0.62-0.83).
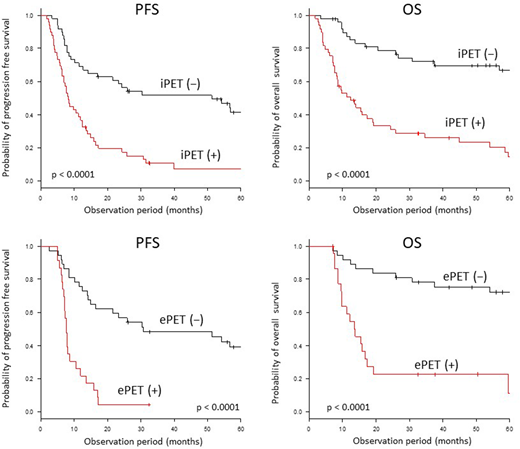
While iPET results were negative in 49 of 98 (50%) cases, ePET results were negative in 35 of 60 (59%) cases. The proportion of patients with PTCL-NOS, AITL, ALCL, ATLL, EATL, CTCL, and NKTCL who achieved CMR with iPET or ePET were 53% (19/36), 82% (23/28), 67% (4/6), 36% (5/14), 50% (1/2), 67% (2/3), and 80% (8/10), respectively. The 5-year PFS and OS were significantly longer in patients with negative results on both iPET (PFS: 41% vs. 7%, p < 0.0001; OS: 67% vs. 15%, p < 0.0001) and ePET (PFS: 39% vs. 0%, p < 0.0001; OS: 72% vs. 11%, p < 0.0001).
Conclusion: These results indicate that iPET and ePET are good predictors of PFS and OS in patients with mature T-cell and NK-cell lymphomas. Furthermore, our findings highlight the significance of iPET findings in the early identification of potential candidates for an intensive therapeutic strategy, with the aim of improving clinical outcomes. Risk-adapted treatment strategies based on iPET and ePET findings should be investigated in larger and prospective clinical trials.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal